
MBBS (AIIMS), MS (Surgery, AIIMS), MNAMS, FACS (USA), FICS (USA), FUICC
Fri, 28 Jul 2023
The first lung transplant was performed in 1963 in USA. Since then, this practice has spread worldwide and the transplant process has evolved manifolds. There have been modifications in the surgical procedure and new technology has been put to use for diagnosis and surgery. This has increased the accuracy of the transplant process and worked in favor of increasing patient survival.
The article below gives you a detailed account of the procedure of lung transplant and what can be expected after this major surgery.
A lung transplant is a major surgery prescribed in cases where the lungs are unable to sustain the life of the individual. This could either be due to a congenital condition, a disease, an injury, infection, chronic inflammation, or other damage. It is worth noting that a transplant is the final option for the doctor and is performed when the patient is not properly responding to any other form of treatment.
This surgery consists of multiple steps involving diagnostic tests, donor search, surgery, recovery, and post-operative care. Considering the vitality of the surgery, the recipient needs to incorporate a healthy lifestyle and habitual changes. Under proper care and precautions, there are higher chances of a successful transplant with a higher life expectancy.
A doctor prescribes a lung transplant only when other treatment methods including medications and therapy do not work. This happens when the lungs have suffered irreversible damage. Due to this, they not only resist treatment but also do not function well enough to sustain the life of the individual. There are several health conditions that can lead up to this. Some of the most common conditions that require a lung transplant include:
For any queries or consultation

This condition involves scarring of the lung tissues. The tissues are irreversibly damaged and become thick and stiff. This disrupts the exchange of gases through the walls of the lungs.
Pulmonary fibrosis is often caused by interstitial lung disease, connective tissue diseases, or long-term exposure to toxic chemicals. This condition is characterized by shortness of breath and chronic dry cough.
This is a condition characterized by the "obstruction" or the partial or complete blockage of the pulmonary channels. It disrupts the airflow through the windpipe and makes it difficult for the person to breathe.
COPD involves diseases like emphysema and chronic bronchitis. The most common symptoms include wheezing, breathing difficulty, dry or wet cough, frequent respiratory infections, and fatigue.
Cystic fibrosis of the lungs involves defect of the mucus clearing mechanism leading to accumulation of mucus plugs, infection, areas of tissue destruction and ultimately fibrosis. The viscid secretions often block the respiratory passages. This condition is characterized by difficulty in breathing, wheezing, and chronic sinusitis.
Pulmonary hypertension refers to the higher than normal blood pressure in the arteries of the lungs that disrupts the exchange of gases through the blood. The obvious cause of secondary to diseases of the heart or lungs. Symptoms include occasional chest pain, chronic cough, and shortness of breath.
A lung transplant could be performed in the form of a single lung, both lungs, or a lobe each of both the lungs. In some cases, this could be combined with transplant of the heart also (Heart Lung Transplant) . Occasionally, it has been combined with kidney transplant also. It depends on the condition of the recipients lungs.
The cadaveric (dead) donors : these are of two types
The human organ transplantation act 1994 (modified in 2014) has defined the brain stem death as death. The brain stem death is to be certified based on clinical parameters and tests to be performed by qualified medical practitioners as defined in the act. So a person who is certified to have brain stem death (hence dead) can be a donor if the family consents for the same.
It is to be clarified that these “Brain dead donors will still have heart beating (which sometimes creates confusion in the minds of the patient’s relatives as the patient being alive). It is to be re- clarified that a person with certified brain stem death is dead as approved by law. This happens in patients of Road Traffic accidents with head injury, stroke and other brain disorders. World wide, this is the largest pool of cadaveric donors and is responsible for the bulk of the cadaveric donor organ transplant activity.
There is a strong need to increase awareness and acceptance amongst the doctors as well as the community at large about the importance of Organ donation in this subset of individuals who are dead (brain stem death) but still have a beating heart. There are large number of such brain stem dead-beating heart ie dead individuals on life support systems in various ICUs across the country and if there was heightened awareness amongst medical community to give the option of organ donation to the family and acceptance of the same by the families, a large number of organ recipients can benefit. One such donor can benefit at least 8 individuals by donating heart, lungs, liver, two kidneys, pancreas, intestines and the two corneas.
These are individuals who have suffered cardiac arrest due to one reason or the other and the organs are donated as soon as possible after the death. These are also known as non-heart beating donors as opposed to the group mentioned above which is known as brain dead-heart beating donors. This may happen in a controlled or an uncontrolled environment. These donors can donate all the above mentioned organs except the heart.
Unlike liver and kidney where living relative donating an organ is the major donation activity in our country, in the case of lungs the same is not possible because donating one lung affects the life of the donor and hence, legally not allowed. Donating a lobe (half part of one lung) is permitted and does not adversely impact the life of the donor but is inadequate to sustain life of the recipient on its own. However, a lobe each from two related donors implanted on either side in the recipient will do no harm to the two donors but will be sufficient for the recipient. This procedure called as “living related bilateral lobar lung transplantation” has ethical issues of two normal people being subjected to a surgery to benefit one individual and has not yet been started in our country. As of today, it is practiced at one centre in Japan on a limited basis.
The steps involved in the lung transplantation process are as below:
The surgery for Lung Transplant tumour can be done best by VATS/Robotic method which has been our speciality for over a decade.
Q. What different lung transplant procedures exist?
Single lung transplants (the replacement of one lung) or double lung transplants (replacing both lungs) are the two main forms of lung transplants. The decision is based on the unique situation and the transplant teams suggestion.
Q. What happens during a lung transplant?
The procedure for a lung transplant is intricate and may last for many hours. The diseased lung or lung(s) is/are taken out during surgery, and the healthy donor lung(s) is/are carefully placed. Patients are initially put on a ventilator and then under strict observation.
Q. What happens after a lung transplant in terms of recovery?
Recovery differs from individual to individual but frequently entails a few weeks in the hospital. To guarantee a positive outcome, medication management, rehabilitation, and routine follow-up care are crucial.
Q. What are the risks and issues associated with lung transplantation?
Risks associated with lung transplant surgery include infection, rejection of the donor organ, and issues with the drugs taken to prevent rejection. Chronic rejection and adverse consequences from immunosuppressive medications are examples of long-term problems.
Q. What is the typical lifespan of a transplanted lung?
While the lifespan of a transplanted lung differs many patients may anticipate that with the right care, the new lungs will continue to function effectively for at least 5 to 10 years, if not longer. Its important to follow up frequently and to take the recommended medications as directed.
Q. Can I decide the time of my surgery for a lung transplant?
Patients typically have little control over when their transplant operation will take place. It depends upon when an appropriate donor organ becomes available as well as once the transplant team determines that the timing is correct to do the surgery. The timing is meticulously planned to guarantee the patients optimal outcome.

Lung Transplant

Prof. (Dr). Arvind Kumar honoured with "Fakhr-e-Hind" (Pride of Nation) award in an International event "Jashn-e-Bharat" organised by Indian Heritage and Health Care Centre and Husanara Trust on 27th January 2019 at India International Centre, Delhi.

A lung transplant is a life-saving and complicate...

Lung transplantation is an extremely sensitive a...

Choosing the best team for a lung transplant can...

A lung transplant is a surgery which is performe...
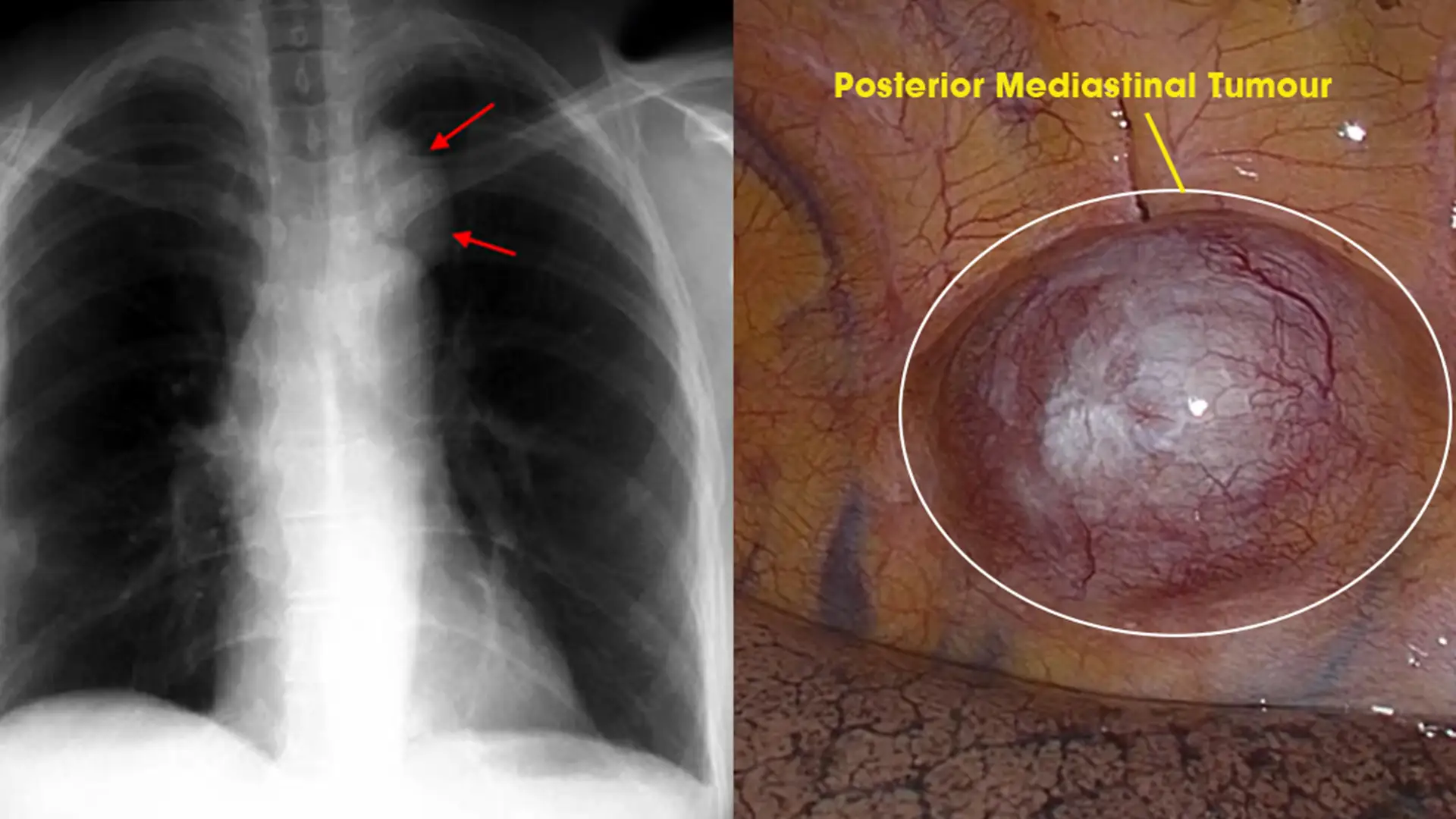
Posterior Mediastinal tumors are benign o...
Copyright @ (Prof.) Dr. Arvind Kumar. All Rights Reserved / Thoracic Surgical Oncologis
License Number: U.P State Medical Council (India) No. 27637


.webp)
 +91-9773635888
+91-9773635888 Contact
Contact